Patients
This study’s protocol was approved by the ethics committee of Nagoya University Graduate School and School of Medicine (No. 2016-0122) and the institutional review board of each institution. Written informed consent was obtained from all patients. All research was performed in accordance with relevant guidelines/regulations, and the Declaration of Helsinki. We prospectively enrolled 74 patients with benign bone tumors or tumor-like lesions for whom a surgical procedure was planned between July 2017 and March 2020. The inclusion criteria were as follows: (1) benign bone tumor or bone tumor-like lesion indicated for surgical treatment, (2) intralesional curettage or en bloc resection followed by filling with Affinos as a bone substitute, (3) availability for radiographs at scheduled time points (preoperative, immediately postoperative, and 1, 2, 3, 6, 9, and 12 months postoperative) and (4) consent for our study. The exclusion criteria were as follows: (1) history of previous treatment with drugs including bisphosphonates, denosumab, and steroids, (2) use of other materials in addition to Affinos during the procedure.
On account of not achieving a follow-up of 12 months after surgery, 16 patients were excluded. Two giant cell tumors of bone recurred during the follow-up period of 12 months: one was in the forearm 8 months after surgery and the other in the proximal fibula 9 months after surgery (Fig. 1). These were not included due to insufficient data and pathological findings. Eventually, 56 patients were eligible and analyzed in this study. Considering the significant small lesions in the fingers and toes compared with those in other bones, the process of bone regeneration in defects filled with Affinos was expected to differ between these bones. Thus, we divided patients into cohort 1 (any bones other than other than phalanges and metacarpal/tarsal bones) and cohort 2 (phalanges and metacarpal/tarsal bones) according to the affected bones, and analyzed the outcomes separately. All procedures described in this study were performed in compliance with the ethical standards set by the Helsinki Declaration of 1975 (revised in 2000) and the regulation of national laws.
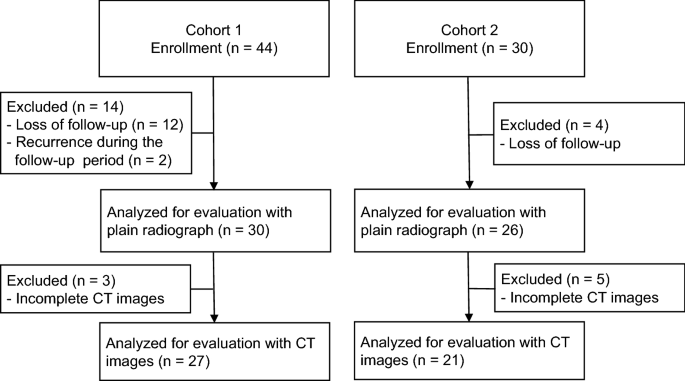
Flowchart of the study patients. CT computed tomography.
Treatment and assessment
Musculoskeletal oncologists performed surgical procedures at each institution. After curettage of the lesion, the defect was loosely filled with Affinos so as not to break its porotic structure. The surgeons individually decided whether to use granular and/or block types for bone defects. They aligned the pore structure of the blocks with the principal strain axis that was experienced in the defect. Prophylactic fixation with locking plates was used in 2 patients with a tibial lesion. En bloc excision was performed in patients with osteoid osteoma. Pathological diagnosis was confirmed by each institutional pathologist. A gradual increase in weight-bearing was allowed during the follow-up period depending on the patient’s symptoms and the radiographic findings. Range of motion exercises was started immediately after surgery.
Radiological evaluation of healing status
Patients underwent evaluation with plain radiographs taken at scheduled time points (preoperative, immediately postoperative, and at 1, 2, 3, 6, 9, and 12 months postoperative). The volume of bone defect was calculated as the product of the anteroposterior, transverse, and cephalocaudal dimensions of a lesion measured on radiographs immediately after surgery9. The cephalocaudal length was measured as the maximum diameter orthogonal to the anteroposterior and transverse dimensions. In order to assess the regeneration process of Affinos in bone defects with radiographic examinations, a semi-quantitative classification was applied based on the five-stage evaluation system of filling materials reported by Anker et al.9,10. Resorption of Affinos and bone trabeculation through the defect were scored as 0%, 25%, 50%, 75%, or 100%. Two independent reviewers (KI and TO), both experienced orthopedic surgeons, evaluated the radiographs. When agreement could not be reached, the score was decided by discussion. Interobserver concordance was assessed by kappa statistic (κ). The degree of agreement for κ-value was interpreted as follows: lower than 0.20, poor; 0.21–0.40, fair; 0.41–0.60, moderate;0.61–0.80, good; and 0.81–1.00, excellent. Patients underwent computed tomography (CT) at 3 and 9 months postoperatively as references for rating the values with plain radiographs. Figure 2 showed an example of assessment of plain radiographs and CT images in determining the values of resorption and trabeculation.
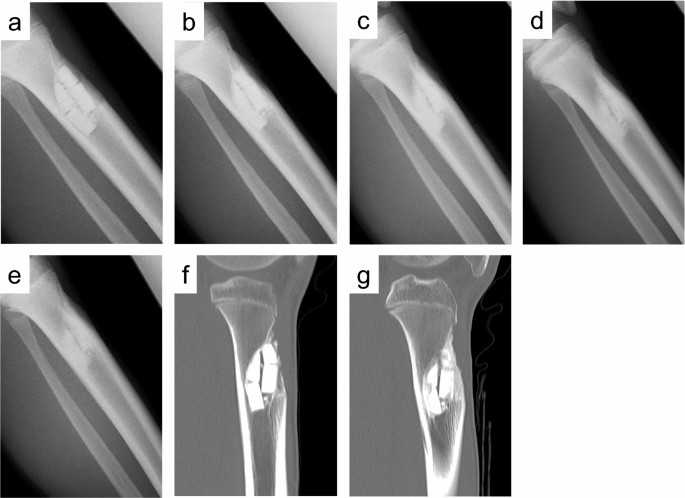
The degrees of Affinos filling the defects were classified into five stages with plain radiographs and computed tomography (CT) images in a 13-year-old boy with tibial fibrous dysplasia. (a) Radiograph at 1 month after surgery: the values of resorption and trabeculation were 0% and 0%, respectively. (b) Radiograph at 3 months after surgery: the values of resorption and trabeculation were 25% and 50%, respectively. (c) Radiograph at 6 months after surgery: the values of resorption and trabeculation were 75% and 75%, respectively. (d) Radiograph at 9 months after surgery: the values of resorption and trabeculation were 75% and 100%, respectively. (e) Radiograph at 12 months after surgery: the values of resorption and trabeculation were 100% and 100%, respectively. (f) Sagittal view of tibial CT at 3 months after surgery: the values of resorption and trabeculation were 25% and 50%, respectively. (g) Sagittal view of tibial CT at 9 months after surgery: the values of resorption and trabeculation were 50% and 75%, respectively.
Bone metabolic markers
To investigate the clinical value of bone metabolic markers regarding the clinical course of healing, we harvested blood samples from 15 patients available for consent. To ensure reliability of blood samples, marker measurements were performed on patients treated at our hospital (Nagoya University Hospital). The levels of bone metabolic markers were measured at baseline (the day after surgery) and 3 and 6 months after surgery. The bone metabolic markers included pyridinoline cross-linked carboxyterminal telopeptide of type I collagen (1CTP) and tartrate-resistant acid phosphatase 5b (TRACP-5b) as bone resorption markers and procollagen type 1 amino-terminal propeptide (P1NP) and bone-specific alkaline phosphatase (BAP) as bone formation markers. Serum TRACP-5b, BAP, 1CTP, and P1NP were measured by SRL Inc. (Tokyo, Japan). The serum level of TRACP-5b was determined with an enzyme immunoassay using the Osteolinks TRAP-5b kit (Nittobo Medical, Japan). Serum BAP was measured with a chemiluminescence enzyme immunoassay method using the Beckman Access Ostase assay kit with a UniCel DxI 800 system (Beckman Coulter K.K., Japan). For the 1CTP assay, the double antibody radioimmunoassay method using a kit provided by Orion Diagnostica (Espoo, Finland) was used, and radioactivity was determined with a γ-counter (ARC950; Hitachi). The double antibody sandwich method was used to measure P1NP with electrochemiluminescence immunoassay using Elecsys total P1NP (Roche Diagnostics, Germany).
Analysis
Statistical analyses were performed using Student t-test for continuous variables. Variables based on repeated observations were compared using repeated measures ANOVA. To evaluate factors associated with the healing status 12 months after surgery, the clinical variables including defect volume, affected bones, gender, the location within the bone (diaphysis, metaphysis, and epiphysis), types of the lesion (cystic vs. solid), and age, as well as radiographical assessments of the values of resorption and trabeculation up to 3 months postoperatively were examined by multiple regression analysis. For categorical variables, multiple regression analysis was conducted with dummy variables. Spearman rank method was used to analyze correlations between the levels of bone metabolic markers and the healing status 12 months after surgery. P-values less than 0.05 were considered statistically significant. SPSS 27.0 for Windows software (SPSS, Inc., Chicago, IL, USA) was used for the statistical analyses.
Ethics approval and consent to participate
This study was approved by the institutional ethics committee of our hospital (No. 2016-0122).