This study included 257 patients who were admitted to our hospital between 2.1.2014 to 29.12.2017, diagnosed with displaced femoral neck fractures and treated with hip hemiarthroplasty.
The patients’ medical files along with relevant radiographs were reviewed. Data on age, gender, comorbidities (hypertension, ischemic heart disease, and diabetes mellitus), pre-injury ambulatory status, duration of surgery, surgical approach, use of a Corail or a Austin-Moore prosthesis, surgeon’s experience and type of anesthesia were collected and analyzed.
Inclusion criteria included patients older than 65 years with a displaced femoral neck fracture, who underwent a hip hemiarthroplasty with either a Corail or an Austin-Moore prosthesis. Exclusion criteria included patients with a pathological fracture, a previous ipsilateral hip fracture or a previous ipsilateral hip fixation.
Radiographs were reviewed and analyzed. Considering that Dorr canal type is an established risk factor for IPF11,12, calcar to canal ratio (CCR) by Dossick and Dorr13, was used to classify femurs. In order to calculate CCR, the femoral canal diameter 10 cm distal to the lesser trochanter was divided by the canal diameter at the mid portion of the lesser trochanter13 (Fig. 1).
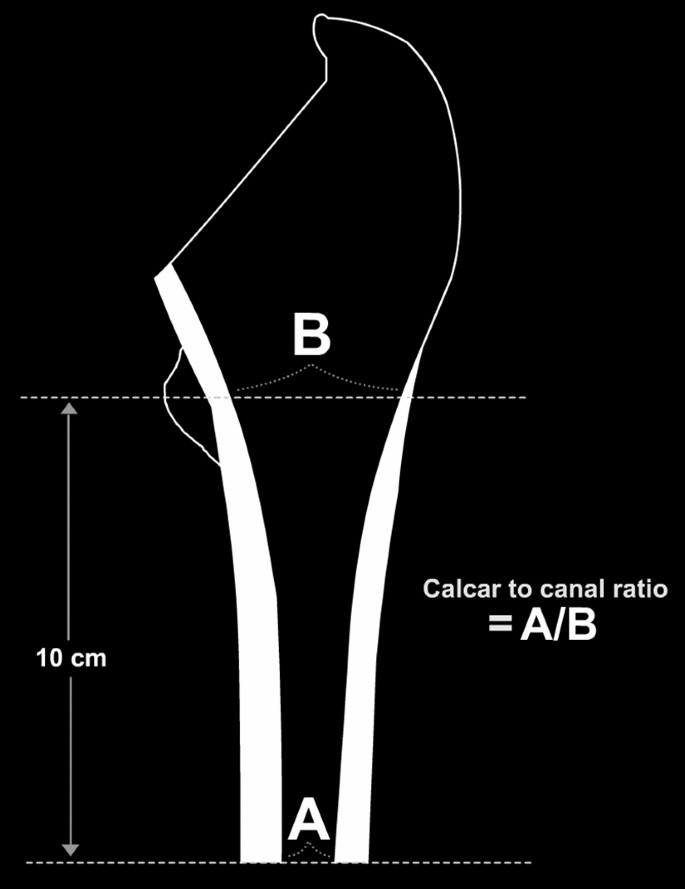
Calcar to canal ratio (CCR) is calculated by dividing the femoral canal diameter at a point 10 cm distal to the mid portion of the lesser trochanter (A) by the femoral canal diameter at the mid portion of the lesser trochanter (B).
Lower values Indicate thicker cortices. Dorr A has a CCR of less than 0.5 and represents a femur with thick cortices starting distal to the lesser trochanter which thicken quickly creating a funnel shaped proximal femur. Dorr B has a CCR between 0.5 and 0.75 and represents a wider femoral canal with some bone loss. Dorr C has a CCR of more than 0.75 and indicates considerable bone loss with thin cortices (Fig. 2).
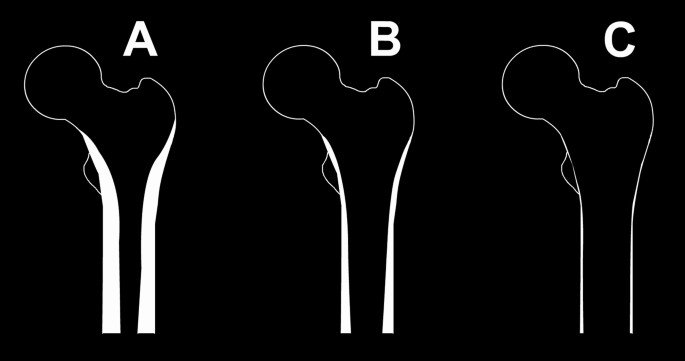
Dorr femur types. Dorr (A) represents a femur with thick cortices and narrow canal. Dorr (B) represents a femur with thinner cortices and a wider canal. Dorr (C) represents a femur with thin cortices and a wide femoral canal.
Femurs were also classified using Canal to diaphysis ratio (CDR). CDR was established formerly as a risk evaluation tool for the occurrence of intertrochanteric fractures14. CDR was calculated by dividing the femoral canal width by the diaphysis width at a point 5 cm distal from the mid portion of the lesser trochanter (Fig. 3). The higher the ratio, the wider the canal, and hence the thinner the cortex. A CDR more than 0.62 indicates that there is high risk for a hip fracture.
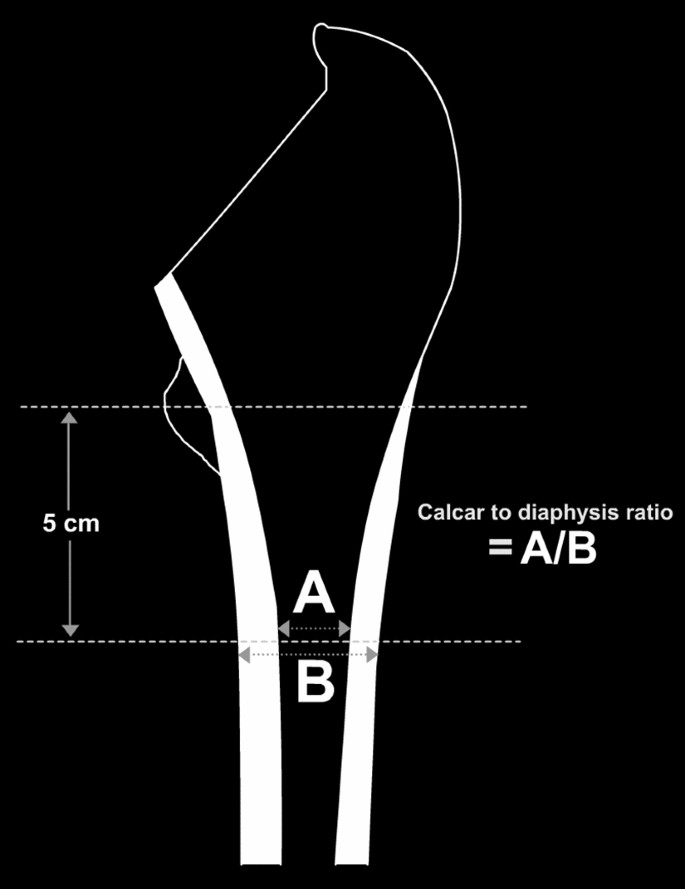
Canal to diaphysis ratio (CDR) is calculated by dividing the femoral canal width at a point 5 cm distal to the mid portion of the lesser (the black arrows) trochanter by the diaphysis width at the same point (the white arrows).
Measurements were taken either on the contralateral femur or on the post-operative ipsilateral femur radiograph due to rotational deformities resulting from the fracture on the admission radiograph.
Preinjury ambulatory status was divided into 4 categories: 1. Freely mobile without aids 2. Mobile outdoors with an aid 3. Mobile mainly indoors 4. Not mobile.
Duration of surgery was recorded in minutes. The three surgical approaches used were the direct lateral (Hardinge), posterior (Moore or Southern) and anterior (Smith-Petersen). Surgical approach was determined mainly by the surgeon’s preference.
Hemiarthroplasty surgery was performed using cementless technique. The prosthesis used were either an Austin-Moore prosthesis (Treu Instrumente GmbH, Tuttlingen, Germany) or a collarless Corail Femoral Stem with a Bipolar Head (Depuy International, Leeds, England).
Our institute shifted from using Austin-Moore to Corail prosthesis with a bipolar head for hip hemiarthroplasty in December 2015. This change enabled us to compare between these two prostheses, by comparing between two different time periods—two years before the era of the Corail prosthesis, and two years after. Patients operated between 2.1.2014 and 20.12.2015 were treated with an Austin-Moore prosthesis, whereas patients operated between 26.12.2015 and 29.12.2017 were treated with a Corail prosthesis.
Surgeons were divided into residents and seniors, whereas seniors are surgeons who completed their residency. Types of anesthesia are general, regional which includes spinal, epidural, or peripheral nerve blocks, and combined anesthesia which includes intravenous combined with regional anesthesia.
In case of an IPF, the following information was recorded if available; 1. The anatomical site of the fracture including greater trochanter, calcar, and anterior femoral neck and lateral femoral cortex. 2. The steps leading to the fracture, including: femoral canal broaching and reaming, trial implant insertion and reduction, and final implant insertion and reduction. 3. The IPF treatment utilized including: cerclage wiring, conversion to a cemented stem, and conservative treatment.
Data entry was performed using a spreadsheet application (Excel 2016, Microsoft Corp., Redmond, WA). Frequency tables and descriptive statistics (mean, standard deviation, Min, Max) were presented for all variables. Categorical variables were presented as proportions and continuous variables were presented as mean. Pearson Chi-Square Test and Fisher’s exact test were used for comparison between categorical variables, while Mann–Whitney U test was used for continuous variables. Statistical significance was set at p ≤ 0.05 and data analysis was performed using SPSS (SPSS Inc., Chicago, IL, Version 27).
As for the statistical analysis, IPF rates were compared between the Corail and the Austin-Moore groups using Fisher’s Exact Test. The univariate analysis tests were used to assess the effects of patient and surgery characteristics on the probability to develop IPF. ROC analysis was performed for CDR and CCR variables to determine the optimal cutoff value and the area under the curve (AUC) was calculated.
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Bioethics Committee of Rambam Healthcare Campus. Our institutional ethics research committee has determined that there is no need for informed consent, as this is a retrospective study.